First a status report! Things are progressing very, very frustratingly slowly. I’m still struggling with pain management. I’ve used up the Percocet that I was prescribed right after surgery. I could request a refill from the doctor but given that it was only marginally effective to begin with I’m switching to acetaminophen (Tylenol). I still have gabapentin and Flexeril, but again, I’m not sure how much those are doing for me other than making me sleepy so I’m only taking them at night. I’m pretty much using the cold therapy machine, which circulates icy cold water through a pad I strap onto my shoulder, constantly except for when I’m doing my PT homework.
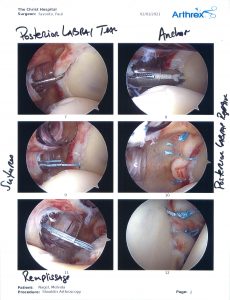
Speaking of PT homework, that’s also frustrating as my motion is extremely limited. To be clear, that’s what we want because the surgeon tightened up my shoulder joint capsule so that it will be stable when all is said and done. But at the moment I can only move it maybe 2 degrees into external rotation and even that tiny motion is very painful. I also can barely shrug my shoulders up toward my ears and even that simple motion is also very painful. So very frustrating! On the other hand I finally got back to acupuncture for the first time since surgery yesterday and actually got a full night of sleep last night for the first time in 2 weeks, so I’ll take that win!
Since I dislocated my shoulder on January 14th and continuing after surgery on February 1st I have had to keep my right arm supported in a sling. Even though it’s my shoulder that’s actually hurt using my right hand is challenging too. That’s because most of the things we use our hand for require stabilization and rotation from the shoulder to get the hand in the optimal position and at the best muscular advantage to complete the task. As my patients like to point out to me, I always say everything is connected. We joke that I should get that painted on my wall so I can just point to it all day. If your shoulder can’t work correctly neither can your hand. (This is also a great illustration of how if you have a hand, wrist, or elbow problem the underlying problem might be a lack of stability and strength at the shoulder!)
Some of the things that are difficult to do with one hand are things that, before this experience, I wouldn’t have even thought about how they’d be affected. In researching how to do things with one hand many of the resources I’ve found are for people who have had amputations or were born with congenital limb differences. These modifications generally use the residual limb to assist with the activity. In the case of an injury like mine you can’t really use the injured side to help at all. So for an injury like mine the modifications are necessarily different and temporary.
I’ve found some good tips and tricks that might come in handy for anyone who, like me, is temporarily unable to use one arm for daily activities due to an injury. Of course for me it’s my dominant hand, which just complicates matters even more!
Handwashing is always essential, but especially important during a global pandemic! It’s challenging with one hand because you can’t use the friction of rubbing your hands together to soap up all surfaces of your hands. What I’ve used to solve this problem is actually meant to be used on the floor of your shower to help you wash your feet. I have it suction cupped to the side of my sink. I get some soap from a pump dispenser in my left hand and then use this to lather up my functional hand.

Dental flossing with one hand is pretty much impossible as far as I can tell with traditional floss. I’ve been using these flossers to keep up what any dentist will tell you is an essential dental hygiene habit even though I can only use my left hand. I also recommend an electric toothbrush, especially if your functional arm is your non-dominant side. That way you can make sure you are still doing a good job of brushing even though you’re using your less coordinated hand.

Washing dishes is difficult with one hand mostly because you normally use one hand to hold the dish in place while you scrub with the other hand. In my case, my husband has been doing most of the dishwashing. We also have a dishwasher so things that can go in there I can just rinse and put in. But sometimes I just want to wash a dish myself or I want a pan or something that can’t go in the dishwasher and I don’t want to bug my husband to do it. After all, he needs to work since one of us needs to be earning money right now! So I got this nonslip mat for the bottom of the sink to hold the dish relatively still while I scrub it with my left hand. I’ve also seen suggestions to use a hammock-like netting across the sink so that the weight of the item being washed holds it still in the fabric hammock. I figure this nonslip mat will be more useful for us in the long run as we can keep using it even after my shoulder recovers. We also have a sprayer on our sink which I’ve found essential for directing higher pressure water where I want it for rinsing.

Staying warm in the middle of winter while wearing a sling is a challenge. This one is admittedly more about wearing a sling than about having one arm to use. Because of the sling I can’t just slide my right arm into a coat. I also can’t really zip up a coat by myself since that’s another thing that you have to stabilize with one hand pulling down while you pull up with the other hand. Luckily ponchos are in style right now. I even saw a hooded, faux fur-lined poncho for sale. I didn’t get that one though as it was a little beyond the price I’m willing to invest.

Also, someone gave me this awesome thing as a gift. The Comfy is basically a giant hoody made out of a fleece-lined velour blanket. I can put The Comfy on over my head and put my left arm through the sleeve and just let the right sleeve dangle empty while my right arm stays in the sling inside it. This thing is super warm, cozy, and big enough that it’s not hard to get it over the sling.

Typing on a computer has been difficult for me. This is something I wouldn’t have thought about before this injury. You would think if it’s just my shoulder affected that typing should be one of the few things that I can still do without any modification. But it’s actually difficult for me to get my right hand turned forward in the right direction to face the keyboard correctly. They do make keyboards that are separated into two pieces, one for each hand, so that you can have your hands in different orientations to the keys. But that’s not an investment I want to make since, as slow and frustrating as this recovery is going to be, it’s not a permanent situation. Also, even if I had the fancy separated keyboard it’s still difficult for me to pronate my right hand (turn it palm down) to type because again, any rotation at the forearm, wrist, and hand doesn’t exist in isolation from a corresponding rotation at the shoulder joint. Therefore, as tedious as it is, I’ve been using my phone to type and also using the voice-to-text feature whenever possible. The phone keyboard is small enough to be used with one hand or with two hands without any pronation of the right arm required.

There are a lot of assistive devices out there to help with doing all kinds of activities of daily living with one hand. Most of them are things I would only get if this was a more long-term or permanent situation or possibly if I lived alone and didn’t have a good support network of folks to help me. For example, just like with washing dishes, cooking is difficult because you would normally have one hand to stabilize the pot while you stir with the other hand. There are pot stabilizers you can get to help with that. There are also food prep boards you can get that have spikes to stabilize something while you chop it with one hand. Click here for a great resource from the UK’s NHS for all kinds of modifications to make activities of daily living easier to do with only one hand.
If you have questions or other ideas that are helpful for doing daily activities with one hand, send me a message or comment on the post on social media. You’ll find me on Facebook @chppt and on Instagram @collegehillppt.